PHRM3101 Week 1 Infection
-
Browse
Uploaded on 2025-01-01 00:00
Describe why microorganisms can be beneficial for health
Microorganisms and its association health
- Often microorganisms are abundant and all around us and are not harmful and in many cases, beneficial and essential for health
- These benefits can include digestion of nutrients to make available for absorption, protection against virulent pathogens, and constant stimulation and strengthening of immune function
Describe how microorganisms cause disease
Microorganisms and its association with disease
Only in some cases
microorganisms are harmful to health. Microorganisms
that cause disease are called pathogens. Severity
of the disease is termed virulence.
These microbes can
exist in low numbers and not cause disease which are termed commensal microbes. The following events can
potentiate disease:
- Overgrowth: Increase in number
- Translocation: Move to another site in the body
- Cross-infection: Transferred to another individual
What types of pathogens are there
Types of Pathogens
Opportunistic: Cause disease when the host's
resistance to the microbe is supressed
(e.g.
immunosuppression due to disease, age, or immunosuppressive medication or
host's microbiota)
Primary: Microorganisms that can cause disease
despite normal host defence
Describe the location of microorganisms in the upper respiratory tract
Upper respiratory Tract: Haemophilus influenzae and Streptococcus pneumoniae are present. If these
are transferred to the lower respiratory tract (aspiration of vomit), they can
be associated with the development of pneumonia
Describe microorganisms on the skin
Skin: If the skin is damaged, Staphylococcus on the skin can invade to cause
cellulitis
Describe the location of microorganisms in the GIT
GIT: Escherichia
coli, if transferred to the urinary tract, can cause UTIs.
Describe the location of microorganisms in the vagina
Vagina: Candida
albicans is normally present in the vagina. Changes in pH or amounts of
other vaginal flora may allow overgrowth of candida and lead to vaginal
candidiasis (thrush)
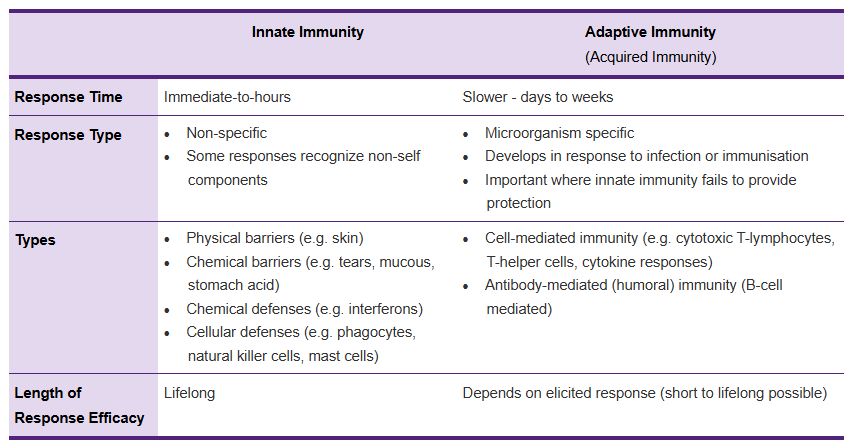
Differentiate innate and adaptive immunity
Describe microscopy as a method of identification of microorganisms
- Microscopy (fast): When a sufficient sample is available, microscopy can immediately be performed to classify bacteria via shape (e.g. cocci, bacillus), and further classified by gram-staining of the bacterial wall (gram-pos/neg/atypical). Combining this information with the infection site and symptoms and usual causative organisms can support initial selection of antibiotic.
Describe Culturing as a method of identification of microorganisms
- Culturing (24hr): Increasing the amount of bacteria for microbial identification. Includes culturing on selective media to determine of bacteria is aerobic or anaerobic or to perform biochemical or mass spec identification. Taking 24hrs, it affects utility for initial selection of an antibiotic
Describe antimicrobial susceptibility as a method of identification of microorganisms
Antimicrobial susceptibility (>24hrs):
Information where antimicrobial susceptibility is requested, culturing in the
presence of a library of antimicrobials needs to be performed (2-3 days). This
guides a prescriber which antibiotics can be used to effectively treat an
infection. Useful where antibiotic resistant microorganisms are present.
Describe PCR as a method of identifying microbes
Polymerase chain
reaction: Amplification and detection of bacterial genes combined with
techniques (e.g. sequencing, micro assays) to identify which bacteria is
present. Fast bacteria identification with small sample amounts and can be used
when microorganisms cannot be cultured.
Describe chest xrays as a method of identifying microbes
Chest X-ray: Useful
for pneumonia diagnosis. Regions that are filled with air are black while
regions that are infected (air sacs filled by pus) appear dense and white
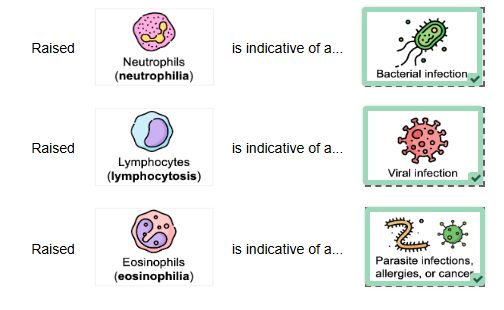
Describe WBC count as a method to identify infection
White
cell count (WCC): WBCs (leukocytes) are important for fighting infections where
the normal range is 4-11 x 109 WCCs/L. Raised levels indicate possibility of
infection but can also indicate other conditions (cancers, inflammatory
conditions). This test provides guidance on what type of microbe is causing the
infection (raised neutrophils indicate bacterial infection)
Describe ESR and CRP as a method to identify infection
Inflammatory
markers: Erythrocyte Sedimentation Rate (ESR) and C-Reactive Protein (CRP) are
raised in response to infection. CRP is produced by the liver and released in
response to inflammation and infection. ESR measures the rate at which RBCs
clump together and sediment which is increased in response to inflammation.
These markers are not specific to infection but is useful to determine if a
confirmed infection is improving.
Describe disk diffusion tests to determine antimicrobial susceptibility
Disk diffusion test: Disks impregnated with
specific concentrations of microbial agents
Describe Etest as a method to determine antimicrobial susceptibility
Etest: Test strips containing a range of
antibiotic concentrations onto bacterial agar cultures
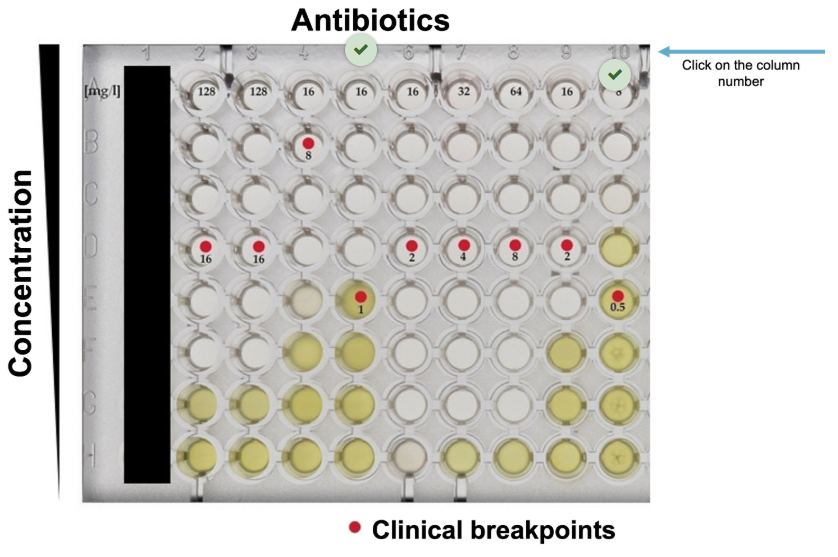
Describe broth (micro)dilution assays to determine antimicrobial susceptibility
Broth (micro)dilution assays: Asses the
capacity for a two-fold dilution series of an antimicrobial to inhibit growth
of a microorganism. Provides minimal inhibitory
concentration data (MIC) which is the lowest concentration of the assessed
antimicrobial that inhibits the overnight growth of a microorganism.
Define bactericidal and bacteriostatic and its relevance to the MIC
- Antibiotics that are able to kill bacteria are bactericidal
- Antibiotics that inhibit bacterial replication are termed bacteriostatic
- At the MIC, some antibiotics will be bacteriostatic while at higher concentrations will display bactericidal activity
The lowest concentration in an MIC assay, which kills
bacteria is called the minimal bactericidal concentration (MBC)
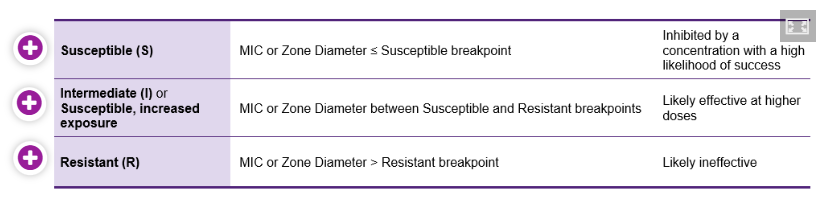
What are breakpoints?
Breakpoints
Breakpoints are
considered to determine if a microbe is susceptible to an antibiotic
What is the reliability of antimicrobial susceptibility tests
Reliability of
antimicrobial susceptibility tests
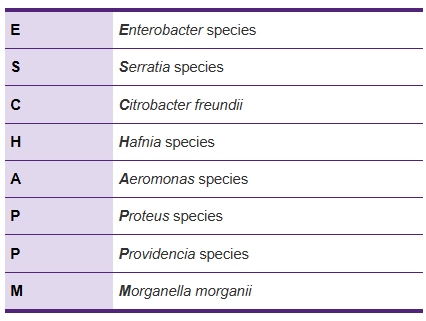
For some
microorganisms, the data from antimicrobial susceptibility tests is not
reliable. The ESCHAPPM pathogens are reported to be susceptible to beta-lactam
antibiotics in these tests, however, they develop resistance rapidly in
clinical practice due to overexpression of an inducible chromosomally encoded
AmpC cephalosporinase. Therefore, many laboratories will report these microbes
as being resistant to cephalosporins. Unlike other beta-lactamase type enzymes,
this enzyme is not inhibited by clavulanic acid.
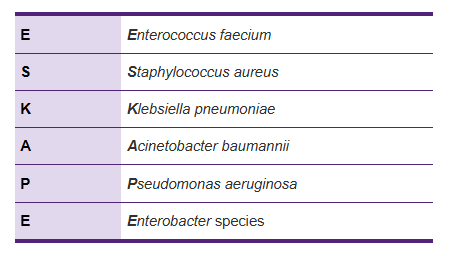
What pathogens are major causes of life-threatening hospital aquired infections associated with increasing rates of resistance to many antibiotics?
ESKAPE Pathogens
Describe the timeline of infection
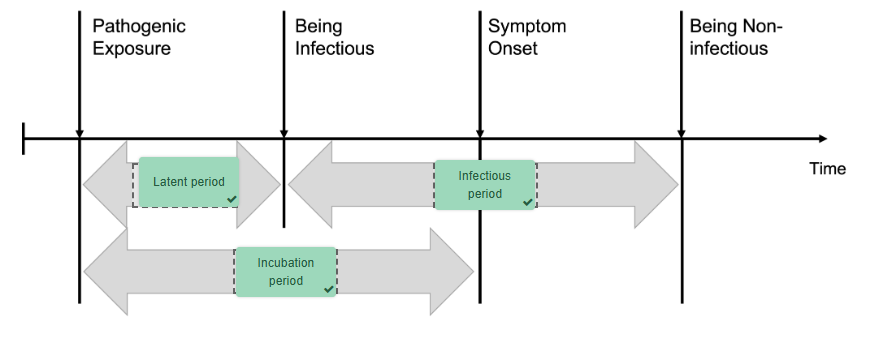
Timeline of infection
Timeframes over
which the host will progress from being infected, to being able to infect
others, displaying symptoms and resolution of symptoms.
Latent period: The period between an individual
being infected with a pathogen and the infection being detectable
Incubation period: The period between the
pathogen invading tissues and the appearance of clinical features of an
infection - longer than the latent period
Period of infectivity (communicability): The
time over which the infected individual is infectious to others. This period
may commence before symptoms of infection are observed, increasing the risk
that the host can infect others.
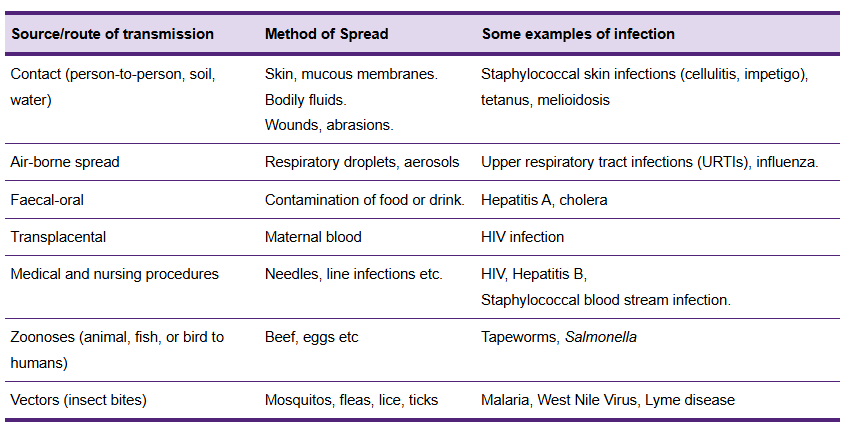
How does the spread of infection occur?
Spread of infection
Spread of pathogens
occur:
Directly: Person to
person or animal to person
Indirectly: Person
comes into contact with an environment contaminated by infected person/animal
What are methods of preventing infection
Preventing the spread of infection
- Handwashing
- Immunisation
- Exclusion of sick individuals (staying away from others - associated with workplaces and facilities and childcare)
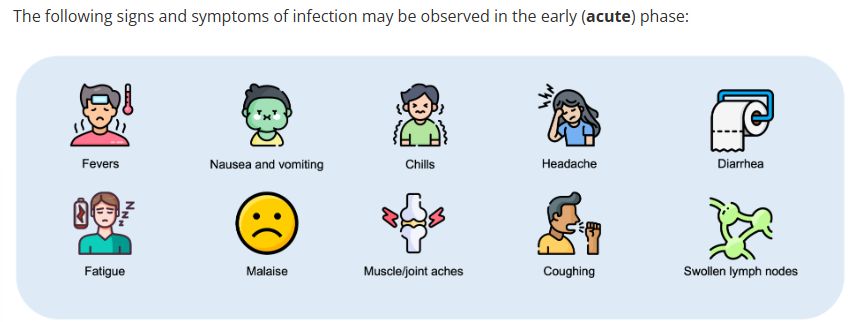
Signs of infection in the acute phase
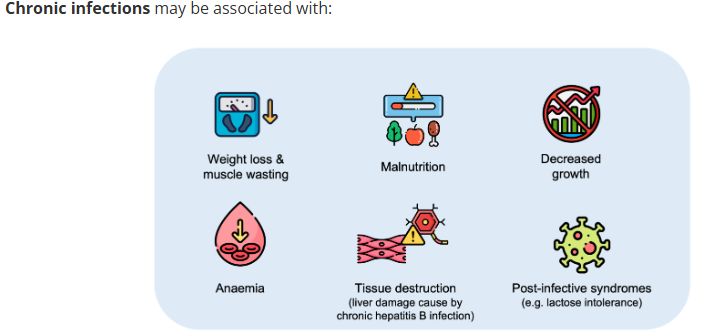
Signs of infection in the chronic phase
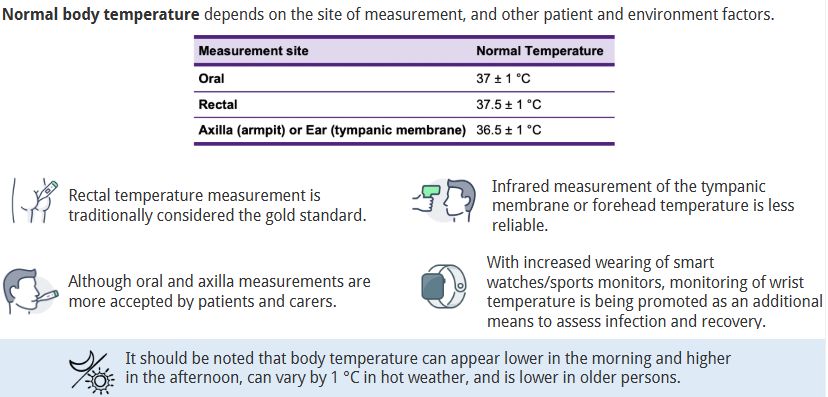
Describe the different methods of taking body temperature
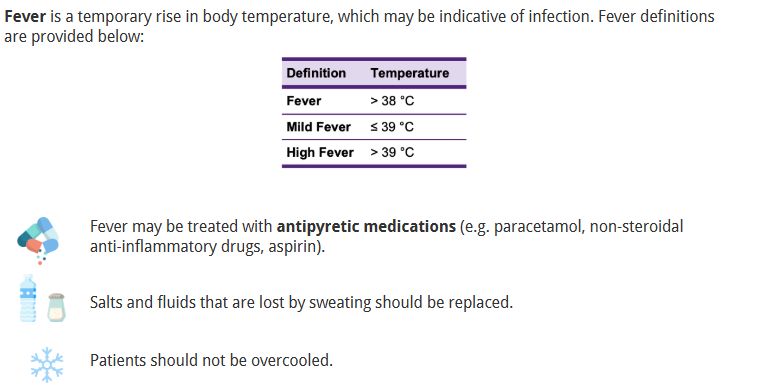
What are the temperatures that are considered a fever, mild fever, or high fever
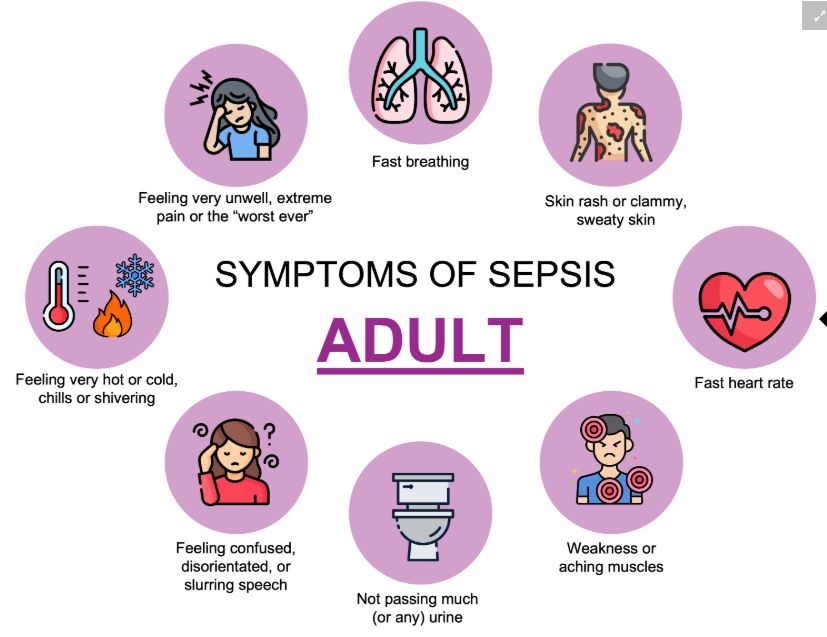
Signs and symptoms of sepsis for adults
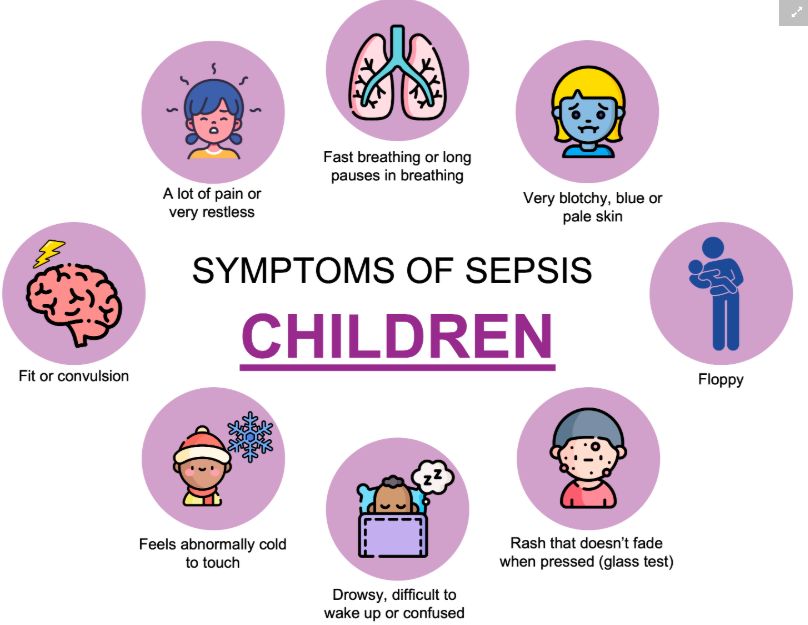
Signs and symptoms of sepsis in children
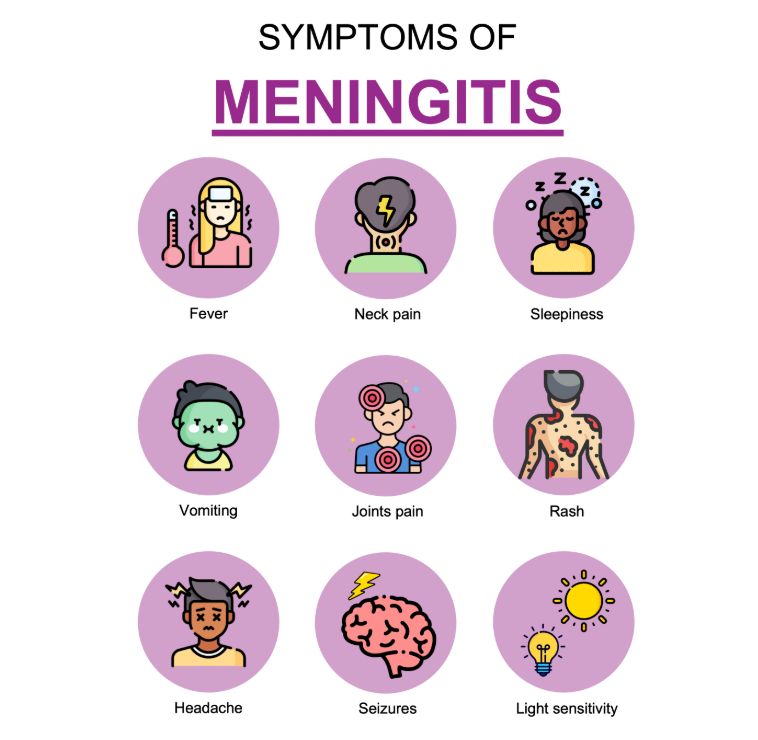
Signs and symptoms of meningitis
Describe what the glass test is
The glass test
Is often described
to investigate for a non-blanching rash (not becoming white). A clear
transparent glass is pressed against the rash. If the rash does not disappear,
this is suggestive of meningitis or septicaemia.
People who show
other signs of meningitis or sepsis but not a non-blanching rash should not
wait to seek medical attention. Shit is time sensitive cuh.
Describe the QUM of antimicrobials for the patient and the healthcare system
QUM of
antimicrobials
For the patient, agents need to be:
For the patient, agents need to be:
- Effective
- Safe
For society and the
healthcare system:
- Avoid antimicrobial resistance
- Cost-effective
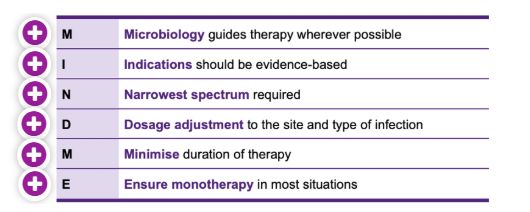
What are the principles for prescribing antimicrobials
What are host-drug interactions
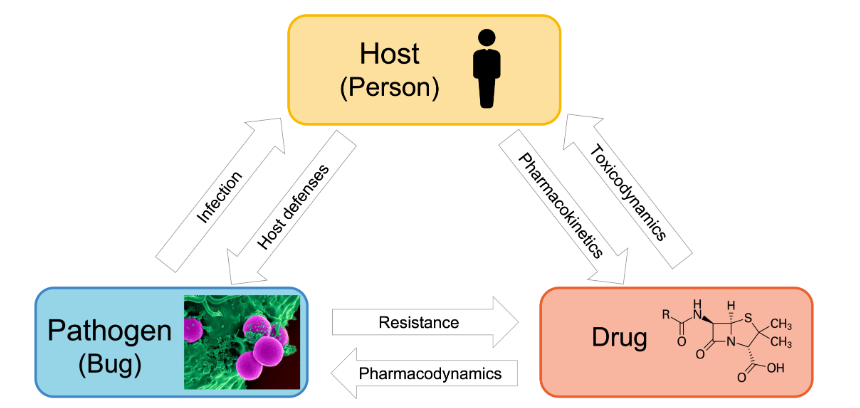
Host-drug
interaction: Patient factors affect pharmacokinetics that cause toxicity or
subtherapeutic outcomes
What are host-bug interactions?
Host-bug
interaction: Infection will have different outcomes on people where immune
response will vary and thus symptoms will present in varying magnitude
What are bug-drug interactions?
Bug-drug
interaction: The drug is trying to inhibit the replication of the bug while the
bus is trying to build resistance to the drug
Describe the prophylactic approach in prescribing antibacterials
Prophylactic
This is where an antimicrobial is used to
prevent an infection from occurring
This method of
antibiotic therapy is restricted to situations where there is a high clinical
risk of infection or infection would be severe.
Surgical prophylaxis is administered to prevent
post-operative infections and involves a single dose of an antibiotic to
achieve high tissue concentrations during surgery.
Non-surgical prophylaxis is administered when:
- Treating contacts of people who have bacterial meningitis or active tuberculosis
- Prevention of rheumatic fever
- Prevention of UTI
- Needlestick injuries
- Prevention of opportunistic infections in HIV infection
Describe the empirical approach to prescribing antibacterials
Empirical
This is when an antimicrobial is selected to
treat an infection based on the most likely and/or important potential pathogen
as well as their antimicrobial susceptibilities. The pathogen has not been
identified.
The clinician will
diagnose an infectious medical condition and consult with appropriate
evidence-based guidelines to decide which antimicrobial to prescribe. Empirical
treatment of infections is the most commonly commenced.
What is directed therapy when prescribing antibacterials?
Directed therapy
This is where a patient has an infection and
the causative pathogen has been identified. This allows selection of an
antimicrobial that is active against the pathogen to be selected. This
however takes time and empirical prescribing may be initially performed.
Directed therapy is
important for life-threatening infections but is not often used where
conditions are normally successfully treated with empirical antimicrobials.
In what cases should combination of antibiotics be prescribed?
Prescribing Combination of Antibiotics
Although antibiotic monotherapy should be used in most situations. There are some cases where combinations can be used.
This is when a patient has an infection that is caused by a mix of pathogens that can't be addressed with a single antibiotic. Synergistic combinations are recommended and in some cases to help prevent development of antibiotic resistance.
What is the synergistic combination of beta-lactams with aminoglycosides?
Beta-lactams with aminoglycosides: Beta-lactam
damages the bacterial wall that allows the aminoglycoside into the bacteria to
inhibit protein synthesis, effectively killing bacteria.
What is the synergistic effect of trimethoprim with sulfamethoxazole?
Trimethoprim with sulfamethoxazole: Both agents
inhibit sequential steps in the bacterial folate metabolism pathway
What is the significance of beta-lactamase inhibitors?
Beta-lactamase inhibitors (e.g. clavulanic
acid, tazobactam or avibactam) may also be administered with beta-lactam
antibiotics (e.g. penicillins or cephalosporins) to reduce their degradation by
beta-lactamase enzymes. They don't have antibacterial activity at clinically
used concentrations but demonstrate synergy when used with beta-lactam
antibiotics - increases antibacterial coverage.
Direct adverse effects of antibiotics
Indirect adverse effects of antibiotics
Indirect adverse effects:
- Candida overgrowth (thrush): Candida overgrowth of the throat and/or vagina can occur
- Clostridioides difficle infection: Overgrowth of C. difficle in the large intestine can result in severe diarrhoea
- Increased colonisation with antibiotic resistant bacteria
Which kinds of antibiotics have more adverse effects?
Adverse
effects are more common with broad-spectrum antibiotics and have greater
effects of the host bacterial microbiome compared to narrow-spectrum
antibiotics.
If monitoring a patient taking aminoglycoside antibiotics, what parameters need to be taken into account?
Monitoring of antibiotic levels
When monitoring a
patient taking aminoglycoside antibiotics:
- Serum creatinine (for eGFR estimation) as aminoglycosides are nephrotoxic
- Concentration monitoring if using for longer than 48 h to maximise antimicrobial effectiveness to reduce toxicity
- Audiometry testing for ototoxicity (hearing and balance). Can cause permanent hearing loss
Concentration
monitoring should not be needed for patients with normal renal function where
aminoglycosides are used for less than 48hrs
What are some causes of antibiotic resistance?
Causes:
- Using antibiotics when they are not indicated (e.g. viral infections)
- Failing to complete antibiotic courses
- Doses that are too low
There is clear
correlation between antimicrobial use and increased antibiotic resistance
What is intrinsic resistance?
- Intrinsic Resistance: Bacteria have properties that make them inherently resistant to an antibiotic (e.g. impermeable, extrude, or enzymatically degrade antibiotics)
What is aquired resistance?
Acquired resistance: Where a spontaneous
mutation or horizontal transfer of resistance genes occurs (more common)
What is transduction in terms of antimicrobial resistance?
Transduction
- Bacteriophages (viruses that infect bacteria) mediate transfer of DNA between
bacteria via transduction. DNA from a
donor bacterium is packaged into a virus particle and transferred into a
recipient bacterium during infection.
What is conjugation in terms of antimicrobial resistance?
Conjugation - The
mechanism of gene transfer most common concerning antimicrobial resistance. A
sex pilus (small ube) forms between two bacterial cells through which a plasmid
is transferred from one to another containing resistant genes.
What is transformation in terms of antimicrobial resistance?
Transformation
- Some bacteria are able to take up free DNA from the environment and
incorporate it into their chromosome
How can you prevent antimicrobial resistance?
Prevention of
antibiotic resistance
- Promotion of wise use of antibiotics
- Improving surveillance of the levels of antibiotic resistance
- Increasing hygiene and infection control
- Investing in development of new antimicrobials
- Raising awareness of issues stemming from the development of antimicrobial resistance
What is the bystander effect when it comes to antimicrobial resistance?
Bystander effect
Unnecessary use of
antibiotics can cause the bystander effect. This is where the use of an
antibiotic both kills the pathogen as well as harmless bacteria. This can
encourage the growth of resistance bystanders that can transfer those resistant
genes to different pathogenic bacteria.
Which antibiotic needs CAL2 prior to dispensing and why?
There is an
exception that the consumption of alcohol should be avoided in patients who are
taking Metronidazole during use and for
up to 24-48 hours after finishing
CAL 2 is applied to these products when dispensing
These interactions
have been described as disulfiram-like interactions, named after the drug
disulfiram used to treat alcoholism. This interaction causes patients to
experience nausea, vomiting, flushing, headaches, and heart palpitations. The
interaction is however proven controversial and evidence of the interaction
lacks.
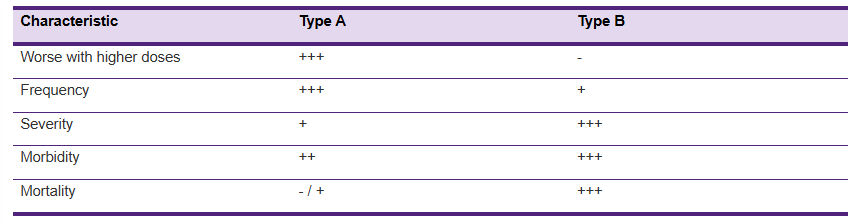
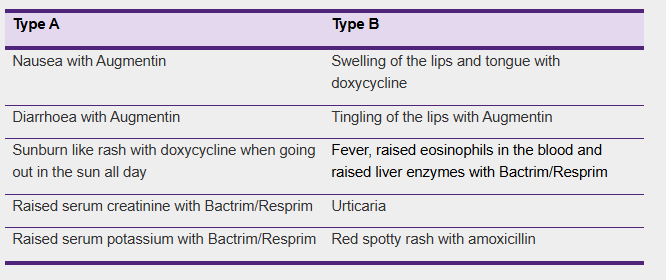
What is the difference between type A and B ADRs?
Hypersensitivity is
a broad term used to describe adverse drug reactions (ADRs).
ADRs are classed
into Type A and Type B:
Type A: Are
pharmacologically predicable reactions
Type B: Include
immediate IgE-mediated and delayed T-cell mediated reactions. Only Type B ADRs
caused by immune-mediated mechanisms should be labelled as 'Allergies'
What are some issues with antimicrobial allergies?
Issues with antimicrobial allergies
If antimicrobials
are dispensed to a truly allergic patient, a severe reaction or even death can
occur. However, many patients who state they are allergic to an antimicrobial
will tolerate the drug if it is taken again.
Penicillins are 1st
line options for the treatment of many infections due to good tolerability and
efficacy. Broad spectrum agents such as quinolones and carbapenems are used
when penicillins cannot be used - as a result, these agents are developing antimicrobial
resistance that can cause no options to treat some patients with infections
- Over 90% of reported penicillin allergies are demonstrated to be not current when patients undergo skin testing or rechallenge with penicillin
- Incorrectly labelling a penicillin allergy costs the healthcare system by forcing clinicians to use more expensive antibiotics
How do you do history taking for someone suspected for antimicrobial allergy
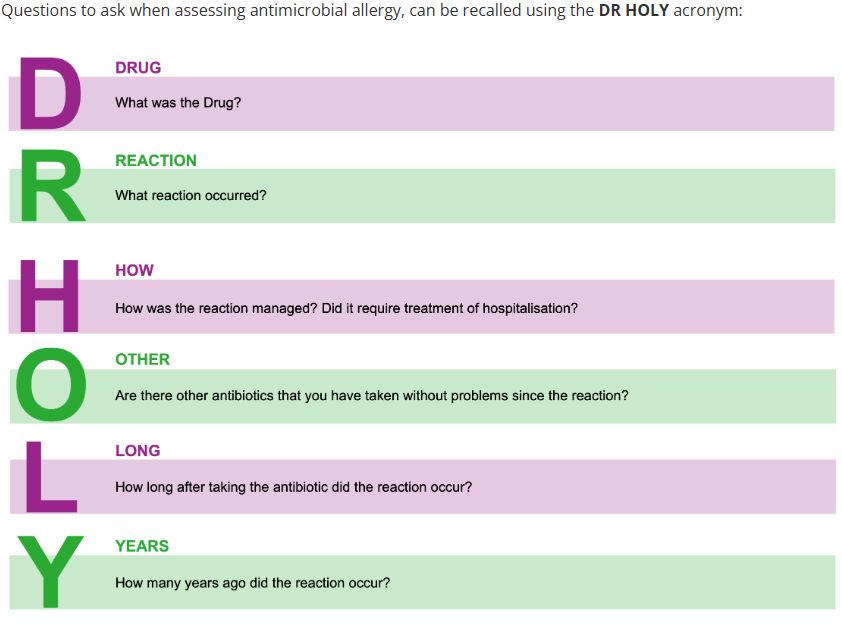
How is a diagnosis of antimicrobial allergy done?
- Clinical history
- Details of reaction
- Timing
- Severity
- Signs such as swelling, SOB, rash
- Physical examination
- Skin testing: small amount of the antimicrobial agent on skin
- In vitro testing to measure IgE antibodies in response to agent
What is a drug challenge?
Drug challenge,
graded challenge or drug test dosing describes careful administration of a drug
in order to see whether a patient is truly hypersensitive. Often used to
confirm tolerance to an antimicrobial when skin-prick or intradermal tests are
negative.
The decision to
rechallenge should be based on severity of previous reaction, the availability
of alternative agents and urgency of infection. To be performed under medical
supervision usually in hospital after consultation with a specialist.
For
people whom a true immune-mediated allergy is not suspected and require
treatment with penicillin but advised the patient has a vague penicillin
allergy label (clinician suspects is not real). A 1/100th or 1/10th dose is
administered and monitored to confirm no allergy. If the challenge is
successful, the label is removed. This challenge is for patients with low to no
risk of true immune mediated reactions. Patients with clear history of immune
medicated reaction or severe cutaneous adverse drug reactions (SCARs) are not
suitable for the drug challenge.
- Appropriate in patients with a history of mild rash in childhood or other delayed non-severe skin reaction
- Prolonged administration for 5-7 days following supervised single-dose provocation is often used to ensure true delayed hypersensitivity is not missed
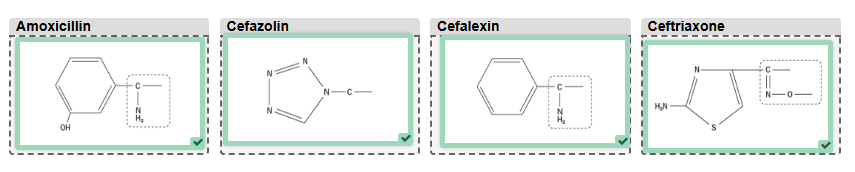
Describe penicillin and cephalosporin cross reactivity
Immune-mediated
reactions from penicillins and cephalosporins are thought to be due to the R1
side-chain that causes an immune response (previously thought to be beta-lactam
ring)
Because penicillins
and cephalosporins have varying R1 side-chains, cross-reactivity can also vary
depending on which agents are prescribed. Penicillins and cephalosporins with
similar R1 chains are likely to have cross-reactivity.
- Amoxicillin has similar R1 chains to cephalexin and cefaclor - likely to have cross-reactivity
- There is common misconception that cephalosporin allergy occurs in approximately 10% of patients who are allergic to penicillin (true figure is 0.2%-2%)
- Cefazolin (used commonly for surgical antimicrobial prophylaxis) has no common side-chains with other beta-lactams and is often tolerated in patients with penicillin or cephalosporin allergies
- Carbapenems are also beta-lactam antibiotics. In patients with penicillin allergy, the rate of cross reactivity is approx. 1%
- Patients with severe penicillin hypersensitivity such as anaphylaxis or angioedema - all penicillins and all cephalosporins are to be avoided
What are the commerically available sulfonamide antibiotics in Australia?
Sulfonamide antibiotics
commercially
available in Australia include:
Sulfamethoxazole: Contains Bactrim, Septrin, or
Resprim. Also contains a second antibiotic called trimethoprim
Sulfadiazine: Not commonly used but is listed
as a treatment option for Toxoplasma gondii (passed from animals to humans)
Sulfacetamide: Antibiotic eye drop
Sulfasalazine: Not used as an antibiotic but
used for IBD such as UC and RA. It is a combination of sulfapyridine
(sulfonamide antibiotic) and a salicylate.
Discuss allergies relating to sulfonamides, namely sulfamethoaxozole and trimethoprim
Allergies relating
to sulfonamides
Up to 8% of
hospitalised patients and 1-2% of those in the community are reported to suffer
an ADR with the combination of sulfamethoxazole and trimethoprim, although 3%
of these are thought to represent hypersensitivity.
Most
hypersensitivity reactions are relatively mild, however, sulfonamides account
for a disproportionate number of cases of life-threatening Stevens-Johnsons
Syndrome and the most severe form of Toxic Epidermal Necrolysis.
In the case a
patient has an allergic reaction to sulfamethoxazole-trimethoprim, there is no
way to determine which API caused it. It is generally assumed to be the
sulfamethoxazole. However both agents should be both avoided if the reaction
was severe.
Labelling someone
allergic to sulfur from a reaction taking a sulfonamide antibiotic is
inappropriate. Sulfur is an element that occurs throughout the human body as a
building block of life and in many foods as sulfates and sulfites. Thus, it is
not possible to be allergic to sulfur itself.
Allergic reactions
to sulfonamide antibiotics do not increase the likelihood of allergy to sulfur
in other forms, including drugs containing the sulfonamide moiety such as
frusemide and celecoxib.
Describe the appropriateness of prescribing a drug (in a different class) with a sulfonamide moiety to a patient known to have an allergy to sulfonamide antibiotics?
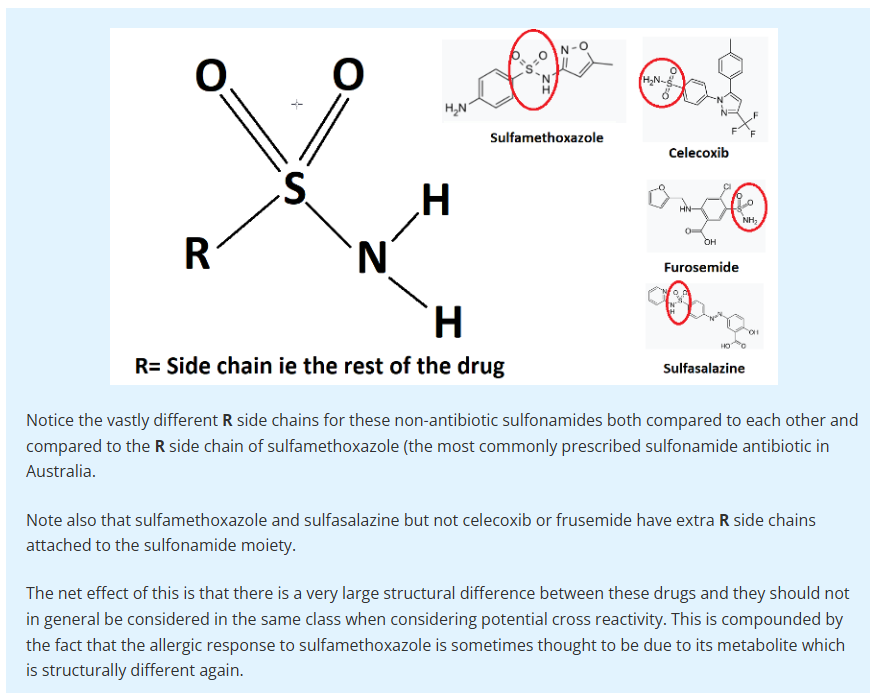
Patients who are
allergic to one antibiotic generally have an increased risk of allergy to any
other antibiotic. Patients with a 'sulfur' allergy can be prescribed another
drug with a sulfonamide moiety from a different class is generally considered
appropriate.
In cases with severe
allergy or ADR (DRESS syndrome, SJS, TENS), drugs with structural similarity
should be avoided (frusemide, bumetanide) - seek specialist advice.
Sulfasalazine breaks down in vivo to release sulfapyridine which is a
structurally a sulphonamide antibiotic, it should not be used in patients who
have severe ADRs related to sulfamethoxazole.
What is desensitisation?
Performed for people
where a true immune allergy is suspected but require treatment with penicillin.
The medication is given in a controlled manner with a small dose (1:10 000)
dilution and gradually increasing the dose to tolerate the medicine without an
allergic reaction. Done when clinical indication for the drug is strong and no
other reasonable options are available.
Not all types of
reactions are safe to undergo desensitisation. Not effective for all types of
reactions. Only recommended for Type-1 (IgE mediated) reactions and not
indicated for severe ADRs
Desensitisation is
temporary. A person is unlikely to have an allergic reaction once desensitised
and continue taking penicillin. Ceasing the antibiotic for more than 24hrs
predisposes the patient makes them at risk for sudden allergic reaction. Do not
remove antibiotic allergy label and write 'desensitised to amox -
/dd/mm/yyyy)'.